Moms and Dads know that when a newborn baby’s skin and eyes appear yellow, they should take them to the doctor. But many of them may not know why. So, what is going on in your baby’s body when this is happening?
When red blood cells have served their purpose and are ready to leave the body, they breakdown and produce a yellow substance called bilirubin. This substance is filtered through the liver and is taken out of the body in your baby’s feces and urine. In a newborn baby there can be several things that cause this bilirubin to build up:
- New babies have more broken red blood cells for a variety of reasons:
- Swallowing Mom’s blood during pregnancy
- Bruising at birth
- Having a different blood type than Mom
- Having an infection
- Having a genetic condition that causes the blood cells to be more fragile
- The liver could not be filtering the bilirubin as it should. Babies born before 35 weeks are at highest risk of this, but it is very common in healthy term babies as well.
- The baby could not be getting enough milk to move the bilirubin out of the body.
If the bilirubin levels stay too high for a long time, then the bilirubin can get absorbed into the brain and cause brain damage. The goal of early recognition and early care is to avoid this condition, called kernicterus.
What to watch for:
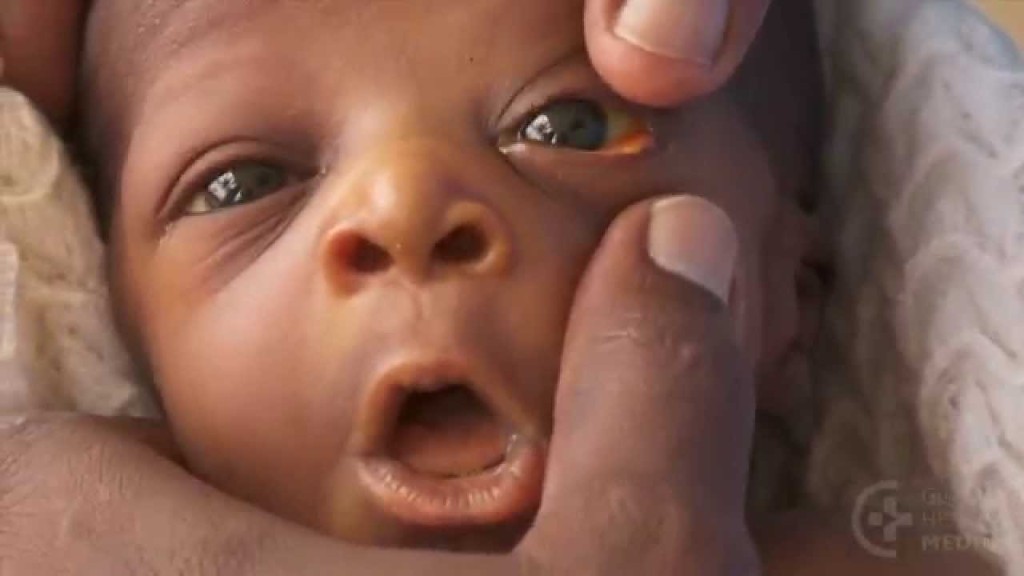
- Do you see yellow in the white parts of your baby’s eyes?
- Is your baby’s skin yellow? For babies with darker skin gently push on the baby’s nose. When you lift your finger, do you see yellow skin?
- Is your baby not feeding well?
- Is your baby not making a lot of wet diapers or do the diapers have dark crystals in them? The goal is 8 wet diapers and 8 feeds in 24 hours.
- Is your baby not making poo diapers? Normal baby poo should be soft and mushy, several times a day for a breastfed baby and daily or every other day for a formula fed baby.
- Is your baby sleeping most of the day? Are you having a hard time waking them up to feed? Do they have a high-pitched cry?
If you have any of the above concerns, you should go to your doctor as they may want to get a bilirubin level. Knowing what to do with the bilirubin results can be a little complicated because care is based on the age of the baby and other conditions. At the American pediatrician’s office where I work now, we use this tool, based on the American Academy of Pediatrics guidelines, to determine the best treatment. I am providing a link here not because I think you should treat your own children, but because this might be a helpful resource for your health care provider:
Treatment may include the following:
- Frequent feeds – Breastfed babies are at highest risk of getting jaundice. The reason is not fully understood. It may have something to do with Mom’s milk supply not coming in early enough, or that the milk may not provide enough bacteria to get the gut working like it should. As bilirubin levels rise babies get sleepier and sleepier and do not appear hungry. Remove some of their clothes, rub the bottoms of their feet, and get them awake to feed. Feed baby every two hours. Your baby may need some bottles of formula to help the body get rid of the jaundice. Be sure the bottles are sterilized and the water has been boiled and cooled before making a bottle. Moms should pump breast milk to help maintain her supply. After a few days and baby is making good wet diapers and is more alert and ready to feed, then return baby to the breast.
- Phototherapy – The light causes the bilirubin to be absorbed into the bowels and will go out of the body with the poo. Of course, baby needs to be feeding well too. The newer phototherapy uses blue light which is most effective. If your baby is under one of the older phototherapy beds, then you’ll need to be sure to keep the eyes protected and stay under the lights as directed. Remove as much clothes as possible.
- Exchange blood transfusions – The goal of early recognition and treatment is to avoid these transfusions that must occur in a neonatal intensive care setting. Some facilities do not have this ability, so if possible, babies with high levels of bilirubin should be evacuated to neonatal intensive care unit. Early recognition, feeding, and phototherapy could avoid evacuations and risk of kernicterus.
